Back pain
Back pain
Overview | Causes | Symptoms | Diagnosis | Treatment | FAQ
Overview
 Back strain is a fairly broad category called “soft tissue
injury,” which covers muscles, tendons and ligaments. About 80%
of back and neck pain is muscle-related.
Back strain is a fairly broad category called “soft tissue
injury,” which covers muscles, tendons and ligaments. About 80%
of back and neck pain is muscle-related.
The stomach muscles, or abdominals, enable the back to bend forward. They also assist in lifting. The abdominals work with the buttock muscles to support the spine. The oblique muscles go around the side of the body to provide additional support to the spine.
Another type of strain relates to spinal ligaments that run in front and in back of the vertebral bodies. Tendons, which also connect muscles in the spine, can develop inflammation, or tendonitis.
Some people believe that part of what makes the back muscles
more prone to strain is that they are shorter than other big muscles
in the body. The muscles in our thighs that enable us to walk, run and
jump are longer and less prone to strain. It’s very unusual to
strain a thigh muscle.
[top]
Causes
Muscles in the back can strain or spasm and form a hard lump, like a
charley horse in the leg. Back muscle spasms can be caused by injury
and pain, whether the source is muscle strain, or a disc problem. A
spasm, defined as an involuntary convulsive contraction of muscle fibers,
can be excruciating. The muscle spasm can be steady or come in waves
of contractions. Your muscle is sending you a signal that it has been
pushed beyond its ability.
[top]
Symptoms
A symptom of muscle strain may be an excruciating spasm in the back that
is very painful.
[top]
Diagnosis
Outlined below are some of the diagnostic tools that your physician may
use to gain insight into your condition and determine the best treatment
plan for your condition.
- Medical history: Conducting a detailed medical history helps the doctor better understand the possible causes of your back and neck pain which can help outline the most appropriate treatment.
- Physical exam: During the physical exam, your physician will try to pinpoint the source of pain. Simple tests for flexibility and muscle strength may also be conducted.
- X-rays are usually the first step in diagnostic testing methods. X-rays show bones and the space between bones. They are of limited value, however, since they do not show muscles and ligaments.
- MRI (magnetic resonance imaging) uses a magnetic field and radio waves to generate highly detailed pictures of the inside of your body. Since X-rays only show bones, MRIs are needed to visualize soft tissues like discs in the spine. This type of imaging is very safe and usually pain-free.
- CT scan/myelogram: A CT scan is similar to an MRI in that it provides diagnostic information about the internal structures of the spine. A myelogram is used to diagnose a bulging disc, tumor, or changes in the bones surrounding the spinal cord or nerves. A local anesthetic is injected into the low back to numb the area. A lumbar puncture (spinal tap) is then performed. A dye is injected into the spinal canal to reveal where problems lie.
- Electrodiagnostics: Electrical testing of the nerves and spinal cord may be performed as part of a diagnostic workup. These tests, called electromyography (EMG) or somato sensory evoked potentials (SSEP), assist your doctor in understanding how your nerves or spinal cord are affected by your condition.
- Bone scan: Bone imaging is used to detect infection, malignancy, fractures and arthritis in any part of the skeleton. Bone scans are also used for finding lesions for biopsy or excision.
- Discography is used to determine the internal structure of a disc. It is performed by using a local anesthetic and injecting a dye into the disc under X-ray guidance. An X-ray and CT scan are performed to view the disc composition to determine if its structure is normal or abnormal. In addition to the disc appearance, your doctor will note any pain associated with this injection. The benefit of a discogram is that it enables the physician to confirm the disc level that is causing your pain. This ensures that surgery will be more successful and reduces the risk of operating on the wrong disc.
- Injections: Pain-relieving injections can relieve back pain and give the physician important information about your problem, as well as provide a bridge therapy.
[top]
Treatment
Surgery is never appropriate for muscle strain.
As with any muscle injury, it’s natural for an individual to stop moving the injured area and wait for it to heal. Ironically, this is counter-productive. Restricting movement causes the muscle to weaken , become less flexible, and receive less circulation. In fact, gentle stretching and exercise is the best way to resolve the injury by getting it moving and increasing circulation.
 Recommendations:
Recommendations:
- Rest.
- Apply ice for five minutes at a time for the first 48 hours, then switch to heat.
- Take anti-inflammatories, preferably ibuprofen like Advil or Nuprin as directed on the bottle. Acetominophen (Tylenol) may be taken for pain, if you are allergic to ibuprofen.
- Try our home remedy exercises. But remember, no exercise should be painful. Stop if they cause an increase in pain or symptoms.
- An appointment with a nonsurgical spine specialist is most appropriate for muscle-related back pain.
- Call us immediately if you experience any emergency, red-flag symptoms.
FAQ
What's the difference between a sprain and a strain?
 While someone may argue that the two words are different, that a sprain
is a more serious injury than a strain, in reality, sprain and strain
have evolved to mean essentially the same things to doctors and lawyers.
Both words relate to an overworked muscle, ligament or tendon that is
overstretched.
While someone may argue that the two words are different, that a sprain
is a more serious injury than a strain, in reality, sprain and strain
have evolved to mean essentially the same things to doctors and lawyers.
Both words relate to an overworked muscle, ligament or tendon that is
overstretched.
Some may argue that strain relates to stretching or tearing of muscles or tendons, while sprain relates to tearing of ligaments or tissues in a joint area. For example, if bones in a joint are forced beyond a comfortable range of motion, the joint may be sprained.
Another word that you may hear is “muscle spasm,” where a muscle locks up in an excruciating, hard lump.
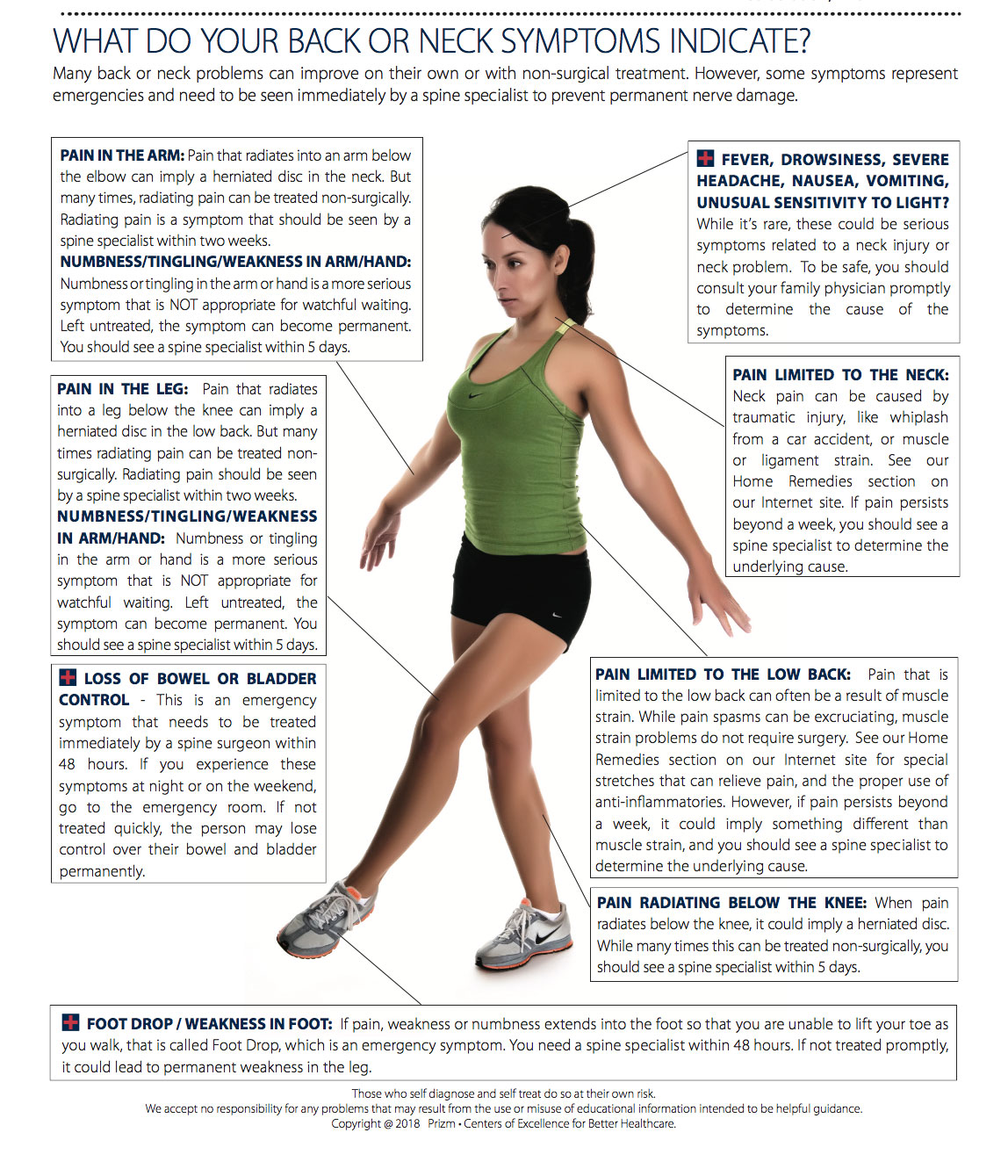
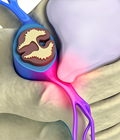
What’s the difference between a simple strain or a more serious herniated disc?
Most people erroneously think that the more excruciating the pain, the
more likely that you herniated a disc. That is not the case at all. In
some cases a back spasm can knock you down to your knees. A person can
have excruciating pain, but if it is mostly in the low back, it’s
probably not a herniated disc. Typically, a herniated disc in your back
will radiate pain down into your leg, or pain will radiate down your
arm if you have a herniated disc in your neck.
[top]
Maahir Haque, MD is recognized as a leader in the field of minimally invasive spine surgery. At Spine Group Orlando, Dr. Maahir Haque, Dr. Ferras Albitar, Dr. José Humberto Jiménez-Almonte, and Dr. Willey also provides second opinions for spine surgery and MRI reviews for those with back pain and neck pain. Dr. Haque emphasizes non-surgical options for back pain and neck pain where possible. This can include accessing a back pain specialist with expertise in pain-relieving spinal injections and spine therapists. Spine therapy can include back stretches that can be a future home remedy for back pain or neck pain. If spine surgery is necessary because of a herniated disc, spinal fracture, or spinal stenosis, Dr. Maahir Haque operates through tubular retractors that reduce the size of the incision, lessen blood loss, reduce time in the hospital, speed return to activity with a less painful recovery. This spine surgery expertise enables many patients to have outpatient spine surgery and be home the same day. Spine Group Orlando provides artificial disc replacement in the neck using the Mobi-C disc implant, the first FDA-approved disc for multiple levels in the neck. Prodisc-C is also used for artificial disc replacement in the cervical spine. Dr. Haque is one of the few spine surgeons in Orlando, Florida to provide lumbar artificial disc replacement using the Prodisc-L artificial disc. Dr. Haque is also referred patients from across Orlando and north central Florida for artificial disc replacement surgery as an alternative to spinal fusion. Accordingly, Dr. Haque's patients travel from across north central Florida, including: Orlando; Jacksonville; Tallahassee; Lakeland; Gainesville; Tampa; Daytona Beach; and Cocoa Beach. The spine center, as a destination for medical tourism for some international patients from Mexico and the Caribbean, can provide recommendations to out-of-town patients on nearby hotels and tourist attractions. Dr. Haque is featured on the national site CentersforArtificialDisc.com as an author on the subject of artificial disc replacement for herniated discs in the neck. The Centers for Artificial Disc web site has content specific to disc replacement options and alternatives to spinal fusion. Click here to visit the Centers for Artificial Disc.